Neoforma Uses Immersive Imaging from Be Here for Groundbreaking Medical Facility Planning Application
Neoforma, Inc. and Be Here Corporation today launched the first-of-its-kind, state-of-the-art virtual reality tour of a medical facility at neoforma.com. Healthcare professionals and medical facility architects around the world can now tour the real world, 1000-room University of Chicago Duchossois Center for Advanced Medicine (CAM) from the convenience of their desktop with Be Here’s immersive images . . .
Neoforma Press Release, July 1998

Panographic image of a medical linear accelerator room
Spinning rooms and not much more.
That was the description that one of our competitors would later use to belittle us. However, I was quite flattered by this characterization. In a time when none of the companies that competed with Neoforma had offered anything original or substantial, we had something quite grand...
That was the description that one of our competitors would later use to belittle us. However, I was quite flattered by this characterization. In a time when none of the companies that competed with Neoforma had offered anything original or substantial, we had something quite grand...
In July 1998, we were only excited by the beauty and value of what we had created. Our competitors would not show up for many months.
I worked for more than a year at Varian before I actually saw one of their cancer therapy machines in a hospital. It was my job to support the customers who purchased these complex machines. I was supposed to help them figure out how to design their hospital to accommodate this big, heavy, radiation-producing equipment and I didn’t have a clue what the rooms really looked like, or how patients and staff interacted in them. Sure, I had seen drawings and photographs of the equipment positioned in a room, but that had given me very little information about what was really in the rooms or what went on in them. This
bothered me. And it gave me an idea.
At Neoforma, we had been trying to figure out how to convert the substantial quantity of traffic at our website into higher quality traffic. That is to say, we wanted to turn our visitors’ activities into revenue opportunities. We wanted people to come to our website every time they were selecting medical equipment. We wanted their experience to be worth the visit. We wanted it to be good.
When a facility is being constructed or remodeled, the vast majority of medical equipment is predetermined. I believed that the best way to service the people who were looking for stuff to put into the rooms of a hospital would be to present our listings of equipment in a hospital setting—not a physical hospital, but a virtual one.
Since early days, when we were producing our CD, we had orga- nized a large database of healthcare equipment, using photographs and three-dimensional drawings of rooms, as well as lists of equipment that went into some of the more complex rooms in a hospital. On the scale we were doing it, this had never been done before. This information was very popular with our customers. If anything, they wanted us to include a broader range of rooms. But there wasn’t any room left on the CD, so we were limited in what we could add.
When we moved this room information to our website, it opened up all sorts of opportunities for improvement. For one thing, since there was no longer a space limit, we could actually present an entire hospital, not just a few departments. And we didn’t have to limit ourselves to one picture per room. It took a lot more information to properly convey what these rooms really looked like.
The problem was that this kind of content was very difficult to get. We had to create the list of products found in each room by commissioning people with experience in each type of room. This was expen- sive and time consuming.
At first, I created three-dimensional computer renderings of a few key rooms. Then we had to commission someone else to do more—also very expensive and time-consuming. It would have been much less expensive to take photos of actual rooms—except a photo couldn’t show as much of the room as a three-dimensional model could. It was while I was searching for a better way to publish this information that I stumbled upon the technology that would give me everything I wanted.
While the presentation stretched the limits of the limited bandwidth and computing power of most Web surfers at the time, panoramic images are really quite simple in concept. They consist of regular photographs with overlapping views of a single scene, electronically stitched together in some way or another and displayed in a window on a computer screen. By moving the mouse around the window, the viewer can pan left, right, up, down and even completely around the scene, giving a very three-dimensional feeling to this two-dimensional window.
The technology was straightforward enough that I was able to mock-up a few Web pages in a couple of days. I was even able to find a way to allow high-quality drawings to be panned and zoomed on the same Web page, using only an Internet browser.
Once I had established the feasibility of these technologies, I was ready to present my idea to the key members of our team.
The idea was that we would select a hospital that demonstrated some of the latest and greatest equipment and design ideas, panoramically photograph every room and hallway, survey every item in every room, gather computer plans of the entire facility, and present it on our website. Every category of every item in about a thousand rooms would be linked to detailed information about the products available and the manufacturers that made them. It would give website unprecedented depth, utility and quality.
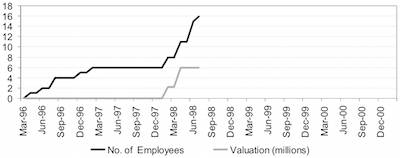
There was some resistance at first, primarily because this seemed like a very ambitious undertaking for a company that employed only sixteen people. Alexander was particularly adamant that all of our efforts should be focused on e-commerce. I expressed my belief that e-commerce functionality wouldn’t do us any good if nobody was using the site as their primary source of information for selecting hospital equipment. When everyone turned to Neoforma for this information, we could support the content by adding contextual advertising too.
The facility I considered to be ideal was the Center for Advanced Medicine (CAM) in Chicago. I had visited it a year earlier and been very impressed by its quality and breadth of services. It was a place that felt more hospitable than most medical facilities I had visited.
CAM wasn’t actually a hospital. It was an ambulatory care center, which means that nobody stayed there longer than twenty-three hours. I thought this was an ideal project because the Center was new, it looked good, it had just about everything a hospital had except the beds, and it was closed most of the weekend. I had calculated that it would take us about forty-eight hours to photograph.
It would be tough to do this while a facility was bustling with staff and patients. At least, I knew I would be uncomfortable if I were a patient — seated in a gown in a waiting room, under stress, in my most introspective and vulnerable moment—if a crew of five obviously-not-from-around-here individuals walked in carrying cameras and clipboards, scurrying this way and that, straightening the furniture and magazines, avoiding eye contact. That could certainly make anybody’s bad day worse.
At CAM, unlike most hospital settings, we could avoid making patients miserable by coming in on the weekend. I figured we could do it with two twelve-hour shifts on two weekends.
After much persistence, I achieved a reluctant consensus on the project.
To do the job in forty-eight hours, we would need four Neoformites: one to set up rooms ahead of us, one to assist the camera person, and two to survey the items in each room. I knew that it would be unfair to expect any of our overworked employees to volunteer to lose two weekends of time with their families, so I volunteered Jeff, Anil and Stephen to join me for duty. After all, they had the most experience with the workings of a hospital. They were thrilled to help out, or so I assumed, since I refused to hear any reason why they might not be able to go.
I had based my time estimate on the use of a specific type of camera to create the panoramic images. Since this technology was quite new and obscure, there were very few choices available for capturing the photos.
One option was to simply stand in the middle of each room and take a bunch of overlapping pictures with a film or digital camera. There was software that could then stitch the images together. However, the number of steps in each room and the difficulty of assembling everything afterward made this option impractical on this scale.
There were a couple of other cameras that spun around and took a single shot for each room, but they didn’t capture a wide enough view for small rooms. We needed the floors and ceilings too.
There was one company that did seem to have what we needed. A venture-backed start-up called Be Here had created a parabolic mirror that fit over a conventional camera. The mirror, which looked like a robot when mounted on its tripod, facilitated the ability to create a single photo which could be converted digitally to an almost spherical view of any room.
I contacted the head of business development at Be Here and told him about what I had in mind. Their primary business model at that point was to sell their cameras for a substantial amount of money. I didn’t intend to spend that kind of money. So in conventional Silicon Valley style, I impressed upon them how groundbreaking our use of their technology would be. I told them that I had been thinking that we should partner to create this first virtual hospital. The PR value to them would be substantial.
I don’t think they entirely bought my argument, but they could tell that I wasn’t going to buy a camera, so they lined up a photographer they had worked with before. She could borrow one of their cameras and we would simply pay for her time and receive a discount on the fees for turning the film images into panoramic images.
This worked fine for me, though I was a bit nervous about the photographer. Most of the photographers I had worked with were very meticulous. I needed someone who could take one image every three minutes, for twelve hours. The Be Here guy assured me that Nancy would be just right for the job.
Now, all I had to do was get permission from CAM and from the architects. I had a great contact at CAM, so I figured it would be an easy task. Who wouldn’t want their facility featured—as a premier example of the best of the best—in way-cool three-dimensional photography?
My contact was Chet Szerlag, who headed up one of the largest departments. I’d met him in my Varian days and had been very impressed with his sincerity, affability and intelligence. I knew that it had been his hard work—before, during and after CAM’s construction — that had been instrumental in making this facility as wonderful as it was. He had become a valued advisor to Jeff and me at Neoforma.
Chet introduced me to the powers that be with his endorsement. But I did not receive the type of reception I had expected.
The first group I spoke with was responsible for hosting visitors to CAM. As one of the newest and most comprehensive ambulatory care facilities in the world, CAM was a very popular destination for hospital executives planning their own new facility or expansion. Pairing tours with educational seminars had become a very profitable enterprise. When I walked in with this idea to publish a tour of their facility online so that anyone in the world could experience their great facility, most of the administrative department members loved the idea. How- ever, the head of the department didn’t. He flatly said no.
He didn’t like the idea of us showing the world what was in each of their rooms. “What if someone saw that we had only three of something and believed that six were required for safety? The liability is unacceptable.”
I told him that we wouldn’t publish the quantities of any item found in the rooms, or even the brand, just what kind of item it was.
Without pause, he moved on to his next argument, “And the way we lay out our rooms . . . what is in them . . . that’s our proprietary information. It’s a big part of how we deliver quality care.”
I made the point that he was already sharing that level of informa- tion with anyone who visited their facility in person. But his biggest issue was that he felt that it might dilute the value of their onsite tour programs. I pointed out that our virtual tour could never replace a physical tour, but it would make more people aware of the facility. And it would deliver the next best thing to those would never be able to visit in person. I thought this argument was persuasive, but his answer was still no.
I was stunned. How could they squelch such a great service to the community? After all, we were going to do almost all of the work. I had been so convinced of the value that this tour would deliver that I had not even considered the possibility that I would be turned down.
I was upset for a few days. Once I had that out of my system, I was set to try another avenue.
I figured that the architects would have very high contacts into CAM, since the executives tend to be fairly active in at least the early stages of projects of this scope. Who would be more eager to get their project published than the architect? Most architects spend a substantial amount of their revenue on marketing activities, particularly on getting their projects published in various periodicals.
I tracked down and contacted Jane, the large architectural firm’s PR person. I gave her my spiel and waited for her enthusiasm. She hesitated, then said, “So, let me get this straight . . . You want to show our building on your website using some new kind of photography? That sounds interesting. And how much are you going to pay us for this?”
I waited for her laugh, indicating that she had only been joking. She didn’t laugh. I could see that things were only getting worse down this path.
But I was getting desperate. And sometimes, when I get desperate, I get pretty good at talking. Luckily, this was one of those times. I took a different tack, explaining to Jane that getting published on our site was indeed an honor, not much different than taking out an ad in a glossy magazine with a large, national circulation. Only, this would be much cooler, reach a much broader audience—and she wouldn’t have to pay thousands of dollars for the photographs.
My expressed desperation had worked. Jane changed her mind. Tentatively, at first, and then with more enthusiasm, she speculated aloud — maybe this would be a good thing, even if they didn’t get paid what they were used to getting paid for. But she had to get the approval of a few people in the local Chicago office. She set up a meeting for me to present the idea to two of the healthcare specialists and the head of the office.
As Jane led me into the appropriately lush, contemporary con- ference room, she apologized, “Tom, our president, won’t be able to join us. He’s on an important call that he thinks will last for longer than this meeting. The rest of us should be able to work through this, though.”
I was disappointed, since I assumed that he was the final decision-maker, but what could I do?
We were soon joined by two men who did not look happy to be wasting their time with me. They had that rushed, distracted look that almost always predicts an unproductive meeting.
It looked like things were taking a bad turn. And then I learned that these were the people primarily responsible for specifying what type of medical equipment would be needed for healthcare projects. When I heard this, my optimism returned. These were exactly the type of people who would benefit from our website.
I gave them a comprehensive briefing and demonstration. Each time I presented the prototypes, I got very excited. This was really cool stuff. I figured that my excitement would be contagious, so I didn’t hold it back.
After I had covered everything, I paused for their comments. One said, “How can you publish all of that information . . . those lists of equipment? We make our living by providing those lists.” The other guy was nodding his head vigorously.
This was not a good sign. I said, “You have to understand. We’ve been publishing this information for years. There is nothing proprietary about lists of what equipment goes in which rooms. Every architect has lists like this. If they don’t, they create them the same way we do— by visiting an actual site.
“Our goal is to make sure that everybody benefits from having complete lists and saves time creating and maintaining them—including you. The value you bring to your clients is the education and experience you use to make the best decisions you can for a particular project—not to republish the list from your last project!”
I had run into this mentality—and been frustrated by it—many times before. It’s my data that makes me so special is an obvious fallacy. As I struggled to make them see that, I know I came on a bit strong. I kept my cool, but refused to yield. They were less cool, but also refused to yield. Jane actually came to my defense several times, but she had little influence with these guys. We were going nowhere.
Just when I assumed all was lost, the president walked in. He fit the part of the senior partner perfectly: grey hair, good suit and a confident, outgoing manner to match. He introduced himself, shook hands with me and sat at the table. “Sorry to be late. I didn’t think I’d ever get off that call! So . . . tell me what this is all about.”
Jane gave him a brief summary of my proposal and voiced her support for it. The specialists voiced their concerns in tense, strained voices. The president listened politely, attentively. When he had heard enough he said, “Okay, let me get this straight. Wayne wants to publish one of our projects on this website of his. If he doesn’t publish one of our projects, he’ll publish one of our competitor’s projects. Is that right, Wayne?”
“Yes, that’s true.”
He stood up, with a look that said how nice it was to have such a short meeting, for a change. “Well, that’s all we need to know.” Turning to Jane, he said, “Give Wayne whatever he needs. Wayne, call Tom at CAM. He’s in charge of their marketing. He’ll make sure you get the approvals you need on their end. Thanks for coming.”
The specialists did not make eye contact with me as I shook their hands and left.
After receiving the permission we needed to photograph the facility, I scheduled two weekend trips to Chicago for our crew. I arranged for us to meet Nancy, the photographer, at our hotel. She would fly directly from her home town in Southern California.
I’m not sure what I expected, but Nancy was definitely not it. A bubbly, casual woman in her thirties, Nancy did not match my stereotype of the neat, serious, professional photographer. That’s probably because she wasn’t. Photography was one of her many hobbies and semi-professions. She ran several websites, one dedicated to the study of UFOs, one to animal rescue, and another to frog memorabilia. She dabbled in Web page design and was taking classes in advanced computer graphics. But most of her notoriety and character had resulted from her position as the host of Zola’s Pleasure Palace, a computer bulletin board dedicated to stretching the boundaries of sexual expression.
We asked Nancy if she preferred to be called Zola. She said that either name was fine, but we could tell she preferred the name of her alter ego. Calling her Zola felt quite natural. She was the last person a casual acquaintance would associate with Zola’s Pleasure Palace. And yet, when you got to know her, the association seemed obvious in some inexplicable way.
I was a bit nervous that she might not be enthusiastic about racing through four 12-hour days. She wasn’t thrilled by the idea of getting up at 4:00 on a Saturday morning, but said she was up for the challenge. And she certainly was.
We arrived at the large, nearly empty facility at 6:00 the next morning. We were greeted by the curious, are-these-guys-nuts?! gaze of sleepy security guards. When I told them why we were there with several cases of equipment, the guard in charge eyed us suspiciously, but acknowledged that he had a note regarding a film crew arriving today. He was clearly nervous about the idea of a group of strangers wandering for hours through rooms filled with all sorts of very expensive equipment. I assured him that we knew what we were doing and wouldn’t disrupt anything.
At first, the security guards had the idea that someone should watch us the entire time, but after an hour or so they realized that we seemed to know our way around a hospital, were terribly boring, and appeared quite focused on our harmless task. So they decided that we would only need a guard around when we entered locked areas. We could just call them on the house phone, they said. But then that happened often enough that they gave up and just let us have a key to get in everywhere, except the pharmacy. Not even the security guards could get into the pharmacy.
So with free access to the entire facility, we methodically documented every room in every department. We wandered through radiology suites, even photographing the MRI rooms—where one false move could send the camera flying toward the magnets, causing tens of thousands of dollars’ worth of damages.
We photographed restrooms and janitors’ closets. We captured the sterile surgical suites wearing booties and hats. Jeff and I couldn’t find the chic, masculine surgeon’s caps we wanted and had to wear slightly embarrassing, blue, muffin-shaped paper bouffants. They did their bit to add to the surreal atmosphere of the empty rooms and corridors.
As we wandered purposefully, hour after hour, we became increasingly aware of the enormity and importance of our task.
In each department, we found the large shelves containing the catalogs of supplies and equipment that each department ordered from. The catalogs were mostly years out of date and represented a very small segment of the current choices in each category. We realized that our site could free up that space and provide so much more current information.
Even though we had all worked in healthcare to varying degrees, we had only an abstract idea of the potential impact Neoforma could have on real people in real hospitals. The creation of this virtual tour solidified our connection to the real thing and gave us a renewed sense that what we were doing wasn’t just good for business, it might actually be important.
As our weariness grew from the grueling work, so did our excitement. There was new meaning and urgency to our work at Neoforma. We really were going to make the world a better place.
We produced many other online tours at notable facilities over the next year, each more interesting and of better quality than the last. The tours became very popular with healthcare providers, designers, and suppliers. They even made some money.
It was ironic, telling, and sad that our competitors would later choose to pick this service to bear the brunt of their criticism. They acted as if adding valuable, educational content to our website was a silly premise for a business, as if it were a sign of weakness.
I worked for more than a year at Varian before I actually saw one of their cancer therapy machines in a hospital. It was my job to support the customers who purchased these complex machines. I was supposed to help them figure out how to design their hospital to accommodate this big, heavy, radiation-producing equipment and I didn’t have a clue what the rooms really looked like, or how patients and staff interacted in them. Sure, I had seen drawings and photographs of the equipment positioned in a room, but that had given me very little information about what was really in the rooms or what went on in them. This
bothered me. And it gave me an idea.
At Neoforma, we had been trying to figure out how to convert the substantial quantity of traffic at our website into higher quality traffic. That is to say, we wanted to turn our visitors’ activities into revenue opportunities. We wanted people to come to our website every time they were selecting medical equipment. We wanted their experience to be worth the visit. We wanted it to be good.
When a facility is being constructed or remodeled, the vast majority of medical equipment is predetermined. I believed that the best way to service the people who were looking for stuff to put into the rooms of a hospital would be to present our listings of equipment in a hospital setting—not a physical hospital, but a virtual one.
Since early days, when we were producing our CD, we had orga- nized a large database of healthcare equipment, using photographs and three-dimensional drawings of rooms, as well as lists of equipment that went into some of the more complex rooms in a hospital. On the scale we were doing it, this had never been done before. This information was very popular with our customers. If anything, they wanted us to include a broader range of rooms. But there wasn’t any room left on the CD, so we were limited in what we could add.
When we moved this room information to our website, it opened up all sorts of opportunities for improvement. For one thing, since there was no longer a space limit, we could actually present an entire hospital, not just a few departments. And we didn’t have to limit ourselves to one picture per room. It took a lot more information to properly convey what these rooms really looked like.
The problem was that this kind of content was very difficult to get. We had to create the list of products found in each room by commissioning people with experience in each type of room. This was expen- sive and time consuming.
At first, I created three-dimensional computer renderings of a few key rooms. Then we had to commission someone else to do more—also very expensive and time-consuming. It would have been much less expensive to take photos of actual rooms—except a photo couldn’t show as much of the room as a three-dimensional model could. It was while I was searching for a better way to publish this information that I stumbled upon the technology that would give me everything I wanted.
While the presentation stretched the limits of the limited bandwidth and computing power of most Web surfers at the time, panoramic images are really quite simple in concept. They consist of regular photographs with overlapping views of a single scene, electronically stitched together in some way or another and displayed in a window on a computer screen. By moving the mouse around the window, the viewer can pan left, right, up, down and even completely around the scene, giving a very three-dimensional feeling to this two-dimensional window.
The technology was straightforward enough that I was able to mock-up a few Web pages in a couple of days. I was even able to find a way to allow high-quality drawings to be panned and zoomed on the same Web page, using only an Internet browser.
Once I had established the feasibility of these technologies, I was ready to present my idea to the key members of our team.
The idea was that we would select a hospital that demonstrated some of the latest and greatest equipment and design ideas, panoramically photograph every room and hallway, survey every item in every room, gather computer plans of the entire facility, and present it on our website. Every category of every item in about a thousand rooms would be linked to detailed information about the products available and the manufacturers that made them. It would give website unprecedented depth, utility and quality.
There was some resistance at first, primarily because this seemed like a very ambitious undertaking for a company that employed only sixteen people. Alexander was particularly adamant that all of our efforts should be focused on e-commerce. I expressed my belief that e-commerce functionality wouldn’t do us any good if nobody was using the site as their primary source of information for selecting hospital equipment. When everyone turned to Neoforma for this information, we could support the content by adding contextual advertising too.
The facility I considered to be ideal was the Center for Advanced Medicine (CAM) in Chicago. I had visited it a year earlier and been very impressed by its quality and breadth of services. It was a place that felt more hospitable than most medical facilities I had visited.
CAM wasn’t actually a hospital. It was an ambulatory care center, which means that nobody stayed there longer than twenty-three hours. I thought this was an ideal project because the Center was new, it looked good, it had just about everything a hospital had except the beds, and it was closed most of the weekend. I had calculated that it would take us about forty-eight hours to photograph.
It would be tough to do this while a facility was bustling with staff and patients. At least, I knew I would be uncomfortable if I were a patient — seated in a gown in a waiting room, under stress, in my most introspective and vulnerable moment—if a crew of five obviously-not-from-around-here individuals walked in carrying cameras and clipboards, scurrying this way and that, straightening the furniture and magazines, avoiding eye contact. That could certainly make anybody’s bad day worse.
At CAM, unlike most hospital settings, we could avoid making patients miserable by coming in on the weekend. I figured we could do it with two twelve-hour shifts on two weekends.
After much persistence, I achieved a reluctant consensus on the project.
To do the job in forty-eight hours, we would need four Neoformites: one to set up rooms ahead of us, one to assist the camera person, and two to survey the items in each room. I knew that it would be unfair to expect any of our overworked employees to volunteer to lose two weekends of time with their families, so I volunteered Jeff, Anil and Stephen to join me for duty. After all, they had the most experience with the workings of a hospital. They were thrilled to help out, or so I assumed, since I refused to hear any reason why they might not be able to go.
I had based my time estimate on the use of a specific type of camera to create the panoramic images. Since this technology was quite new and obscure, there were very few choices available for capturing the photos.
One option was to simply stand in the middle of each room and take a bunch of overlapping pictures with a film or digital camera. There was software that could then stitch the images together. However, the number of steps in each room and the difficulty of assembling everything afterward made this option impractical on this scale.
There were a couple of other cameras that spun around and took a single shot for each room, but they didn’t capture a wide enough view for small rooms. We needed the floors and ceilings too.
There was one company that did seem to have what we needed. A venture-backed start-up called Be Here had created a parabolic mirror that fit over a conventional camera. The mirror, which looked like a robot when mounted on its tripod, facilitated the ability to create a single photo which could be converted digitally to an almost spherical view of any room.
I contacted the head of business development at Be Here and told him about what I had in mind. Their primary business model at that point was to sell their cameras for a substantial amount of money. I didn’t intend to spend that kind of money. So in conventional Silicon Valley style, I impressed upon them how groundbreaking our use of their technology would be. I told them that I had been thinking that we should partner to create this first virtual hospital. The PR value to them would be substantial.
I don’t think they entirely bought my argument, but they could tell that I wasn’t going to buy a camera, so they lined up a photographer they had worked with before. She could borrow one of their cameras and we would simply pay for her time and receive a discount on the fees for turning the film images into panoramic images.
This worked fine for me, though I was a bit nervous about the photographer. Most of the photographers I had worked with were very meticulous. I needed someone who could take one image every three minutes, for twelve hours. The Be Here guy assured me that Nancy would be just right for the job.
Now, all I had to do was get permission from CAM and from the architects. I had a great contact at CAM, so I figured it would be an easy task. Who wouldn’t want their facility featured—as a premier example of the best of the best—in way-cool three-dimensional photography?
My contact was Chet Szerlag, who headed up one of the largest departments. I’d met him in my Varian days and had been very impressed with his sincerity, affability and intelligence. I knew that it had been his hard work—before, during and after CAM’s construction — that had been instrumental in making this facility as wonderful as it was. He had become a valued advisor to Jeff and me at Neoforma.
Chet introduced me to the powers that be with his endorsement. But I did not receive the type of reception I had expected.
The first group I spoke with was responsible for hosting visitors to CAM. As one of the newest and most comprehensive ambulatory care facilities in the world, CAM was a very popular destination for hospital executives planning their own new facility or expansion. Pairing tours with educational seminars had become a very profitable enterprise. When I walked in with this idea to publish a tour of their facility online so that anyone in the world could experience their great facility, most of the administrative department members loved the idea. How- ever, the head of the department didn’t. He flatly said no.
He didn’t like the idea of us showing the world what was in each of their rooms. “What if someone saw that we had only three of something and believed that six were required for safety? The liability is unacceptable.”
I told him that we wouldn’t publish the quantities of any item found in the rooms, or even the brand, just what kind of item it was.
Without pause, he moved on to his next argument, “And the way we lay out our rooms . . . what is in them . . . that’s our proprietary information. It’s a big part of how we deliver quality care.”
I made the point that he was already sharing that level of informa- tion with anyone who visited their facility in person. But his biggest issue was that he felt that it might dilute the value of their onsite tour programs. I pointed out that our virtual tour could never replace a physical tour, but it would make more people aware of the facility. And it would deliver the next best thing to those would never be able to visit in person. I thought this argument was persuasive, but his answer was still no.
I was stunned. How could they squelch such a great service to the community? After all, we were going to do almost all of the work. I had been so convinced of the value that this tour would deliver that I had not even considered the possibility that I would be turned down.
I was upset for a few days. Once I had that out of my system, I was set to try another avenue.
I figured that the architects would have very high contacts into CAM, since the executives tend to be fairly active in at least the early stages of projects of this scope. Who would be more eager to get their project published than the architect? Most architects spend a substantial amount of their revenue on marketing activities, particularly on getting their projects published in various periodicals.
I tracked down and contacted Jane, the large architectural firm’s PR person. I gave her my spiel and waited for her enthusiasm. She hesitated, then said, “So, let me get this straight . . . You want to show our building on your website using some new kind of photography? That sounds interesting. And how much are you going to pay us for this?”
I waited for her laugh, indicating that she had only been joking. She didn’t laugh. I could see that things were only getting worse down this path.
But I was getting desperate. And sometimes, when I get desperate, I get pretty good at talking. Luckily, this was one of those times. I took a different tack, explaining to Jane that getting published on our site was indeed an honor, not much different than taking out an ad in a glossy magazine with a large, national circulation. Only, this would be much cooler, reach a much broader audience—and she wouldn’t have to pay thousands of dollars for the photographs.
My expressed desperation had worked. Jane changed her mind. Tentatively, at first, and then with more enthusiasm, she speculated aloud — maybe this would be a good thing, even if they didn’t get paid what they were used to getting paid for. But she had to get the approval of a few people in the local Chicago office. She set up a meeting for me to present the idea to two of the healthcare specialists and the head of the office.
As Jane led me into the appropriately lush, contemporary con- ference room, she apologized, “Tom, our president, won’t be able to join us. He’s on an important call that he thinks will last for longer than this meeting. The rest of us should be able to work through this, though.”
I was disappointed, since I assumed that he was the final decision-maker, but what could I do?
We were soon joined by two men who did not look happy to be wasting their time with me. They had that rushed, distracted look that almost always predicts an unproductive meeting.
It looked like things were taking a bad turn. And then I learned that these were the people primarily responsible for specifying what type of medical equipment would be needed for healthcare projects. When I heard this, my optimism returned. These were exactly the type of people who would benefit from our website.
I gave them a comprehensive briefing and demonstration. Each time I presented the prototypes, I got very excited. This was really cool stuff. I figured that my excitement would be contagious, so I didn’t hold it back.
After I had covered everything, I paused for their comments. One said, “How can you publish all of that information . . . those lists of equipment? We make our living by providing those lists.” The other guy was nodding his head vigorously.
This was not a good sign. I said, “You have to understand. We’ve been publishing this information for years. There is nothing proprietary about lists of what equipment goes in which rooms. Every architect has lists like this. If they don’t, they create them the same way we do— by visiting an actual site.
“Our goal is to make sure that everybody benefits from having complete lists and saves time creating and maintaining them—including you. The value you bring to your clients is the education and experience you use to make the best decisions you can for a particular project—not to republish the list from your last project!”
I had run into this mentality—and been frustrated by it—many times before. It’s my data that makes me so special is an obvious fallacy. As I struggled to make them see that, I know I came on a bit strong. I kept my cool, but refused to yield. They were less cool, but also refused to yield. Jane actually came to my defense several times, but she had little influence with these guys. We were going nowhere.
Just when I assumed all was lost, the president walked in. He fit the part of the senior partner perfectly: grey hair, good suit and a confident, outgoing manner to match. He introduced himself, shook hands with me and sat at the table. “Sorry to be late. I didn’t think I’d ever get off that call! So . . . tell me what this is all about.”
Jane gave him a brief summary of my proposal and voiced her support for it. The specialists voiced their concerns in tense, strained voices. The president listened politely, attentively. When he had heard enough he said, “Okay, let me get this straight. Wayne wants to publish one of our projects on this website of his. If he doesn’t publish one of our projects, he’ll publish one of our competitor’s projects. Is that right, Wayne?”
“Yes, that’s true.”
He stood up, with a look that said how nice it was to have such a short meeting, for a change. “Well, that’s all we need to know.” Turning to Jane, he said, “Give Wayne whatever he needs. Wayne, call Tom at CAM. He’s in charge of their marketing. He’ll make sure you get the approvals you need on their end. Thanks for coming.”
The specialists did not make eye contact with me as I shook their hands and left.
After receiving the permission we needed to photograph the facility, I scheduled two weekend trips to Chicago for our crew. I arranged for us to meet Nancy, the photographer, at our hotel. She would fly directly from her home town in Southern California.
I’m not sure what I expected, but Nancy was definitely not it. A bubbly, casual woman in her thirties, Nancy did not match my stereotype of the neat, serious, professional photographer. That’s probably because she wasn’t. Photography was one of her many hobbies and semi-professions. She ran several websites, one dedicated to the study of UFOs, one to animal rescue, and another to frog memorabilia. She dabbled in Web page design and was taking classes in advanced computer graphics. But most of her notoriety and character had resulted from her position as the host of Zola’s Pleasure Palace, a computer bulletin board dedicated to stretching the boundaries of sexual expression.
We asked Nancy if she preferred to be called Zola. She said that either name was fine, but we could tell she preferred the name of her alter ego. Calling her Zola felt quite natural. She was the last person a casual acquaintance would associate with Zola’s Pleasure Palace. And yet, when you got to know her, the association seemed obvious in some inexplicable way.
I was a bit nervous that she might not be enthusiastic about racing through four 12-hour days. She wasn’t thrilled by the idea of getting up at 4:00 on a Saturday morning, but said she was up for the challenge. And she certainly was.
We arrived at the large, nearly empty facility at 6:00 the next morning. We were greeted by the curious, are-these-guys-nuts?! gaze of sleepy security guards. When I told them why we were there with several cases of equipment, the guard in charge eyed us suspiciously, but acknowledged that he had a note regarding a film crew arriving today. He was clearly nervous about the idea of a group of strangers wandering for hours through rooms filled with all sorts of very expensive equipment. I assured him that we knew what we were doing and wouldn’t disrupt anything.
At first, the security guards had the idea that someone should watch us the entire time, but after an hour or so they realized that we seemed to know our way around a hospital, were terribly boring, and appeared quite focused on our harmless task. So they decided that we would only need a guard around when we entered locked areas. We could just call them on the house phone, they said. But then that happened often enough that they gave up and just let us have a key to get in everywhere, except the pharmacy. Not even the security guards could get into the pharmacy.
So with free access to the entire facility, we methodically documented every room in every department. We wandered through radiology suites, even photographing the MRI rooms—where one false move could send the camera flying toward the magnets, causing tens of thousands of dollars’ worth of damages.
We photographed restrooms and janitors’ closets. We captured the sterile surgical suites wearing booties and hats. Jeff and I couldn’t find the chic, masculine surgeon’s caps we wanted and had to wear slightly embarrassing, blue, muffin-shaped paper bouffants. They did their bit to add to the surreal atmosphere of the empty rooms and corridors.
As we wandered purposefully, hour after hour, we became increasingly aware of the enormity and importance of our task.
In each department, we found the large shelves containing the catalogs of supplies and equipment that each department ordered from. The catalogs were mostly years out of date and represented a very small segment of the current choices in each category. We realized that our site could free up that space and provide so much more current information.
Even though we had all worked in healthcare to varying degrees, we had only an abstract idea of the potential impact Neoforma could have on real people in real hospitals. The creation of this virtual tour solidified our connection to the real thing and gave us a renewed sense that what we were doing wasn’t just good for business, it might actually be important.
As our weariness grew from the grueling work, so did our excitement. There was new meaning and urgency to our work at Neoforma. We really were going to make the world a better place.
We produced many other online tours at notable facilities over the next year, each more interesting and of better quality than the last. The tours became very popular with healthcare providers, designers, and suppliers. They even made some money.
It was ironic, telling, and sad that our competitors would later choose to pick this service to bear the brunt of their criticism. They acted as if adding valuable, educational content to our website was a silly premise for a business, as if it were a sign of weakness.

 RSS Feed
RSS Feed